Contributing author: Lars Johansson (Chief Scientific Officer @ Antaros Medical)
Weight loss induces some degree of muscle loss. This is true across lifestyle, surgical, and pharmacological interventions and is not a new concept. But with the degree of weight loss that can be achieved with this new generation of anti-obesity medications (AOMs), changes in body composition, especially those related to muscle, have become increasingly important for interpreting treatment effects within drug development.
So, why is it biologically, functionally and clinically relevant to look at muscle changes with weight loss? How can we assess muscle composition and function in clinical trials using imaging and other methods? And how can these insights support decision-making throughout drug development and help differentiate therapies beyond weight loss?
Niels Jessen (Head of Research at Steno Diabetes Center, Aarhus), Tim Heise (Chief Scientific Officer at Profil) and I tried to answer some of these questions and address these topics in a webinar called ‘Underneath the lost kilos: muscle composition, preservation and function’. This blog post will summarise some of what we spoke about; focusing on why we should and how we can look at changes in muscle during weight loss.
Why look at muscle?
Historically, clinical trials generally only reported weight loss in absolute (e.g. kilograms) or relative (%) terms. With today’s approved weight loss compounds and those currently in development, their unprecedented weight loss effects have led to a need for better understanding what the weight loss represents and how much of it is coming from fat. There is also a whole class of drugs that are focusing on both weight loss and muscle preservation.
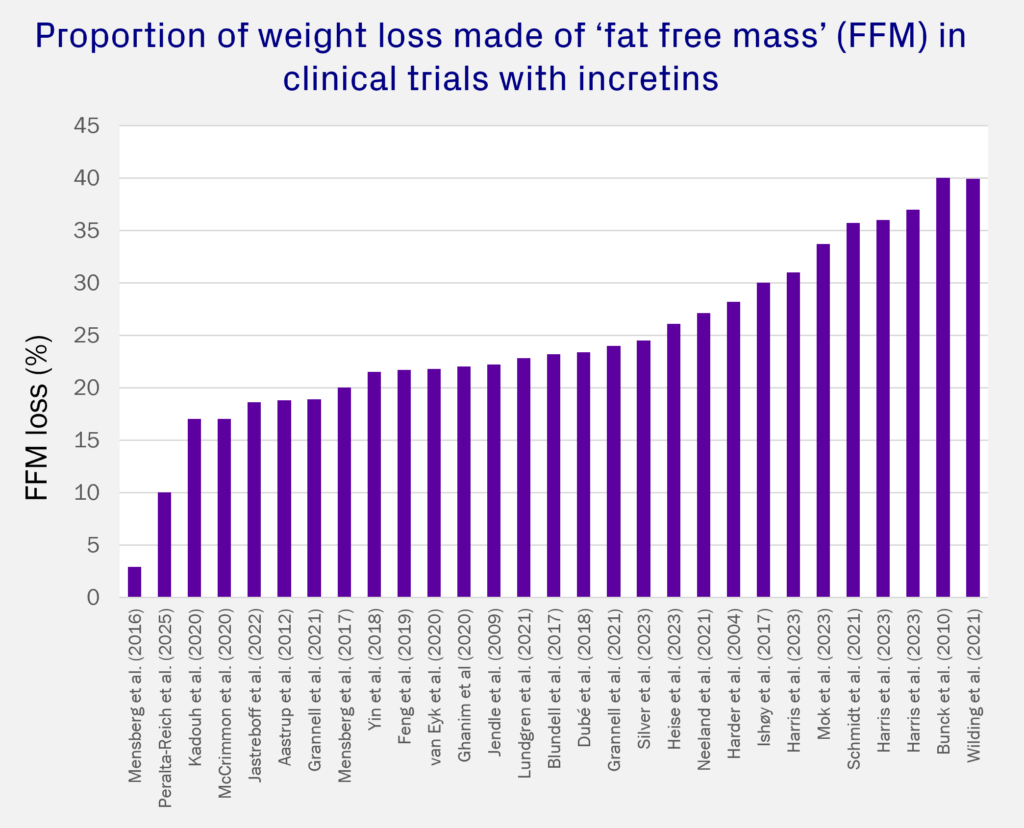
This has led to a number of trials measuring body composition, and reporting loss of ‘fat free mass (FFM)’ during weight loss. FFM includes essentially everything that isn’t fat, such as bone, water and muscle. Even with different trials of the same drug and dose, there is a lot of variability in the reported proportions of weight loss that are FFM (See Figure 1). While some of this variation could be due to differences in treatment effects, other aspects like patient population characteristics, trial duration, and method of measurement will have a significant impact on these results, and should be kept in mind when interpretating data.
It is important to note is that FFM is not a direct measure of muscle, even though they are sometimes used interchangeably, as muscle is only a part of FFM. Furthermore, adipose tissue contains FFM, approximately 15% of adipose tissue is water. The two commonly used methods to report FFM are bioelectrical impedance analysis (BIA) and dual-energy X-ray absorptiometry (DXA), which measure water and lipids, respectively, and calculate FFM from there. Magnetic resonance imaging (MRI), on the other hand, measures muscle directly. To read more about the differences between DXA and MRI for body composition, check out this blog post by some of my colleagues.
However, what has become even more important to look at is muscle function. There is of course going to be less concern about loss of muscle mass if there is not detrimental effect on muscle function.
Muscle biology and function
The defining cell type of skeletal muscle is the muscle fiber. Each muscle is made up of a combination of 3 different fiber types, which can be classified in different ways, most commonly into slow oxidative (Type 1), fast oxidative (Type 2a), and fast glycolytic (Type 2b). There is a lot of heterogeneity and variation both between people and between muscles when it comes to muscle size and composition of fiber types, which are influenced by age, genetics, physical training, etc.
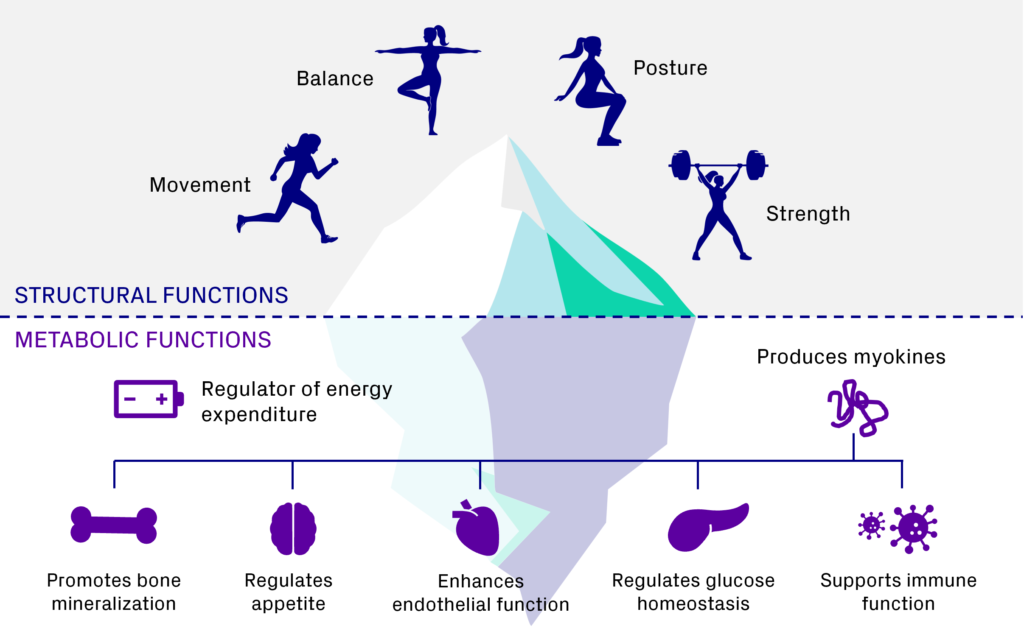
Most discourse about muscle function focuses on its physical and structural functions like movement, balance, posture, and strength, but skeletal muscle also has many important metabolic functions. Skeletal muscle mass is the main determinant of energy expenditure and regulator of glucose homeostasis. Muscle also produces myokines, which are signaling molecules that serve as endocrine factors and communicate with other organs. This in turn supports immune function, regulates appetite, and enhances endothelial function, among other things.
Muscle is also a very dynamic tissue. Most of what we know about how muscle changes comes from studies in cachexia, muscular dystrophies and the effects of ageing. With age, even in healthy people, we see that muscle mass slowly declines, and this slightly precedes a steeper decline in muscle strength.
What changes with obesity?
Certain disease states, such as obesity, can accelerate or exacerbate changes in the muscle. Some key changes are:
- Increased fat accumulation
- Development of chronic inflammation and formation of fibrosis
- Impaired mitochondrial function and protein synthesis,
- Impaired glucose uptake and development of insulin resistance
- Reduced physical performance
- Fiber type shifts.
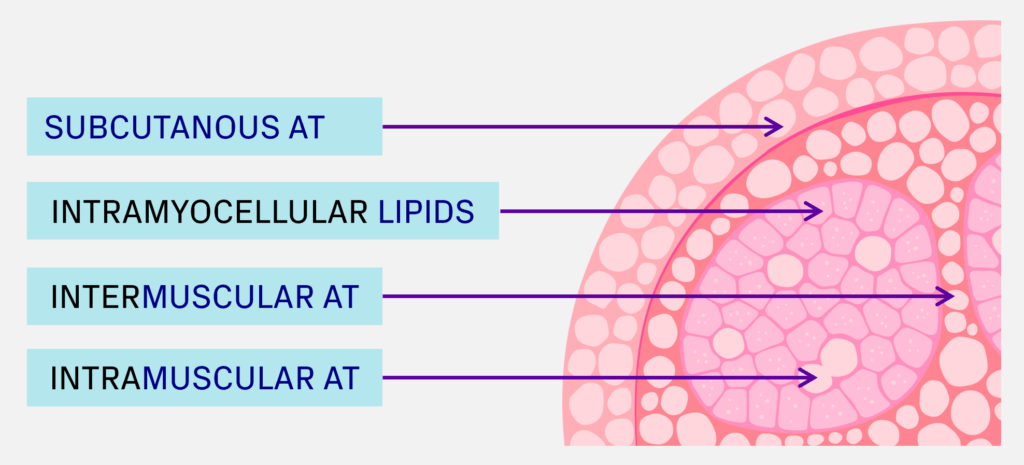
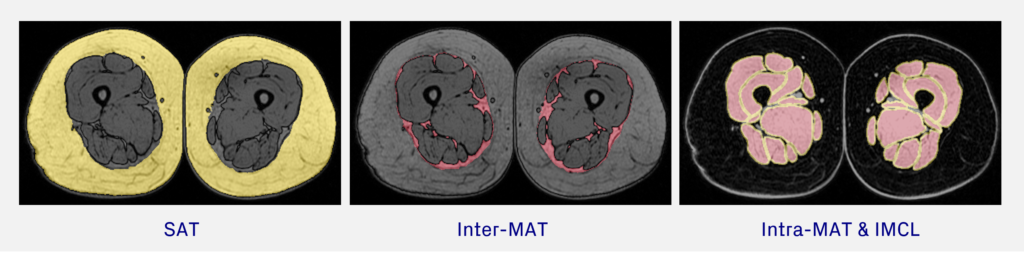
Muscle fat can be further classified based on its location (See Figure 3). Subcutaneous adipose tissue (SAT) is located outside of the muscle, whereas intermuscular adipose tissue (inter-MAT) is located beneath the deep fascial layer, surrounding the muscles. Intramuscular adipose tissue (intra-MAT) is within the muscle, between muscle fibers and fascicles. Finally, intramyocellular lipids (IMCL) are lipid droplets stored within the muscle cells. You can read more about the different muscle fat types and muscle composition here.
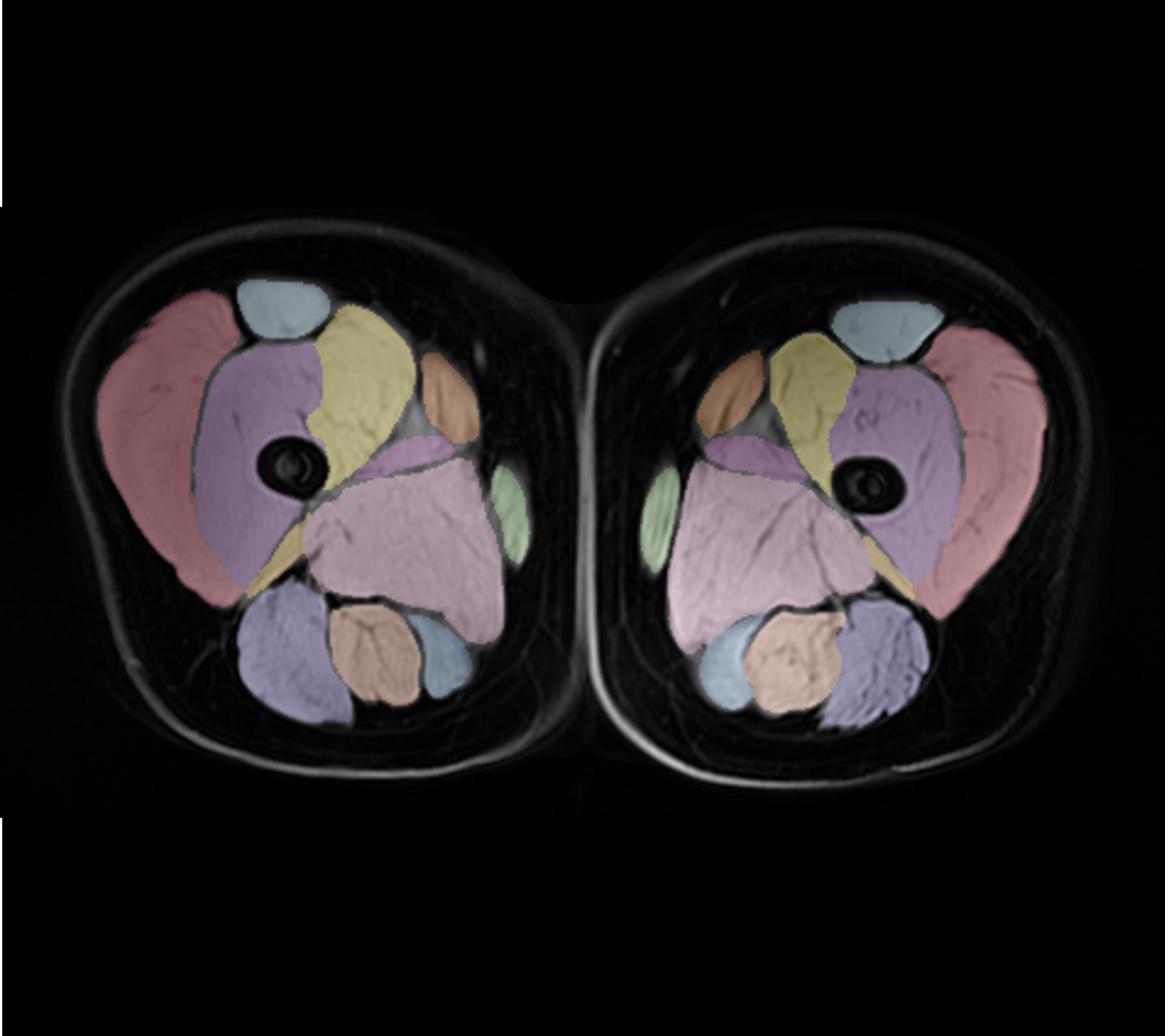
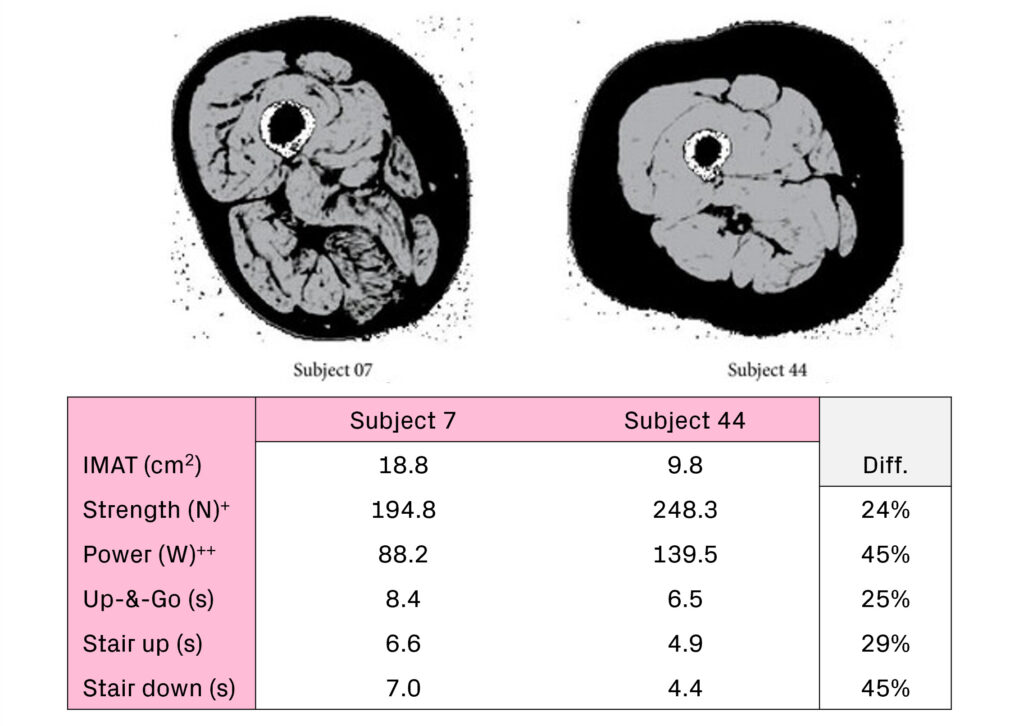
All these different muscles changes are linked. In Figure 4, you can see MRI images of 2 women matched for age, body mass index (BMI), and lean muscle mass. One has twice the amount of intermuscular adipose tissue, and significantly impaired physical function as measured by knee extension strength, lower extremity power, etc.
Measuring changes in muscle composition and function
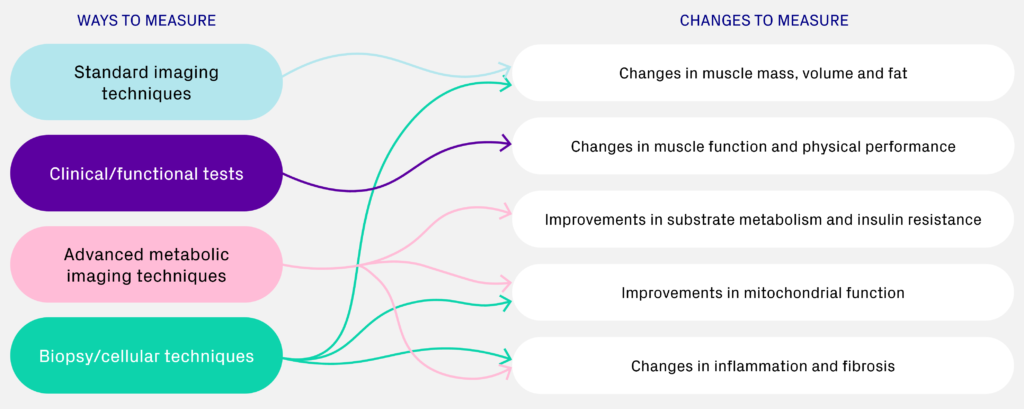
There are a number of methods and ways to measure different types of changes in muscle composition and function. Here, I’ll just discuss measuring changes in muscle volume and fat with MRI, and changes in muscle function and physical performance with clinical tests. For examples of the other types, you’ll need to watch the webinar.
Measuring muscle composition with MRI
The advantage of using MRI and segmenting each individual muscle is that you can directly measure muscle volume, and you can quantify the different types of muscle fat, namely subcutaneous adipose tissue (SAT), inter-MAT, and intra-MAT, making it possible to measure fat-free muscle volume. The individual muscle fat fraction also varies a lot between different muscles.
Measuring muscle function and physical function with clinical tests
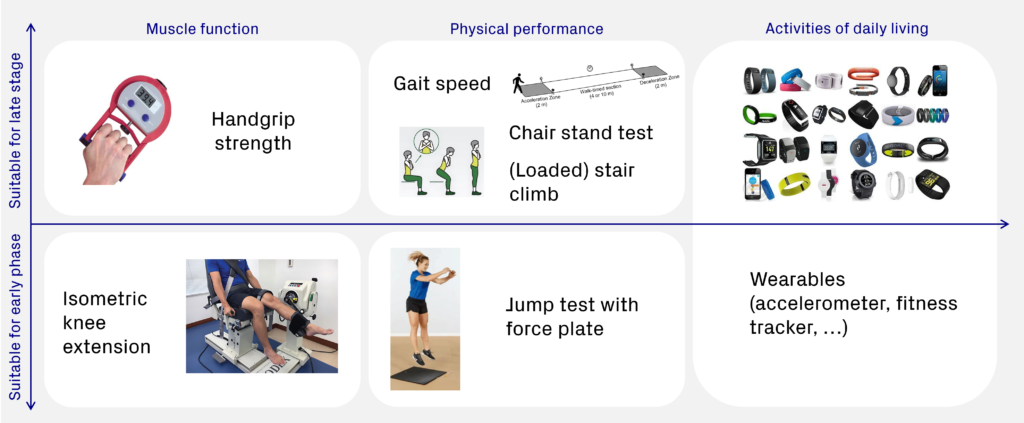
There is a so-called ‘Hierarchy of loss of physical function’ as proposed by Beaudart et al., which suggests that first there is loss of muscle function, which has 3 elements; strength, power and endurance. Then there is loss of physical performance and mobility, which are measured as movements that involve other organs and systems. And ultimately, there is impact on activities of daily living,
There are hundreds of muscle function and physical performance tests, and variations, and no real gold standard. Some are easier to measure, making them more suitable for later phase trials (e.g. handgrip strength). It is worth noting that in trials for obesity, this becomes more difficult, as patients generally still have pretty good physical performance compared to those with sarcopenia. So, for these patients, you might need more sensitive tests, but the increased level of sophistication limits their suitability for larger trials.
Implications for drug development and future outlook
We are starting to see some obesity clinical trials include measures of muscle function. This started in obesity-related heart failure with preserved ejection fraction (HFpEF) populations, where in addition to looking at body weight, physical performance as measured by 6-minute walk test (6MWT) was also reported (e.g. in STEP-HFpEF, SUMMIT). In the case of the HuMAIN trial, body composition, muscle volumes and fat were also studied.
More recently, there have been trials that have looked deeper into functional changes in addition to changes in body weight and body composition. The BELIEVE trial included measures of handgrip strength, and the SemVLCD study reported on changes in handgrip strength and knee extension strength. I think this is only the beginning of more and more trials including measures of muscle function and physical performance.
This is also on the radar of the major regulatory bodies, who have already included advice regarding body composition to their guidelines for weight loss drug development. Both the FDA and EMA ask that body composition is reported to ensure that effective weight loss (>5%) is reflecting primarily a reduction in fat. However, drugs focusing on muscle preservation may not reach this threshold for effective weight reduction, and instead have been advised to demonstrate clinically beneficial preservation of physical function. At this stage, I don’t think anyone really knows exactly what this looks like, but there is certainly more work to be done here.
Closing thoughts
To summarize briefly what has been covered in this blog post, it is biologically and clinically relevant to look deeper into muscle cellular, compositional and functional changes in weight loss trials. This is for a number of reasons:
- To better understand the large variation seen in the proportion of non-fat weight loss in clinical trials. Interpretation of results should always take into consideration patient population characteristics, trial duration, and method of measurement in addition to the drug’s mode of action.
- To ensure that the clinical benefit of weight loss is also seen in terms of muscle function. Looking solely at mass negates whether there are other beneficial changes in the muscle that are more important for physical performance and metabolic health.
- To paint a more complete picture of muscle changes and treatment effects by integrating different methods that can combined in different ways to answer different biological and mechanistic questions.
Blog disclaimer:
The views and opinions expressed in this article are solely those of the contributing author/s. These views and opinions do not necessarily represent those of Antaros Medical.
Contact details:
If you have any questions regarding this article, please reach out to press@antarosmedical.com