
Contributing authors: Moritz Schneider (Senior Director MR Imaging) and Henrik Haraldsson (Senior Director MR Imaging) @ Antaros Medical
The obesity drug development landscape is evolving quickly and there are many compounds in development with the shared goal of inducing weight loss for the treatment of overweight/obesity and other metabolic diseases. Incretin-based therapies, in particular glucagon-like peptide-1 (GLP-1) receptor agonists, have shown unprecedented weight loss in obesity. However, for both market differentiation and regulatory purposes, it is increasingly important to demonstrate the ‘quality’ of weight loss and a meaningful, lasting health impact.
This means that in clinical trials, it’s not just about how much weight is lost – but what that weight loss actually represents. Is it adipose tissue or lean mass? Where in the body is it coming from? And how does it affect muscle quality, organ health, metabolic resilience and physical function?
Imaging methods can unlock these deeper insights through enabling assessments of body composition. In clinical trials, the most commonly used imaging methods for body composition are dual-energy X-ray absorptiometry (DXA; or sometimes shortened to DEXA) and magnetic resonance imaging (MRI). Each method has its advantages and disadvantages, offering insights into different aspects related to body and muscle composition. They can also vary regarding availability, technical and operational complexity, and the level of insights they can provide.
There is no one-size-fits-all approach when it comes to imaging that will work for every trial. However, if you know your key research questions, then they, along with your developmnent phase, will guide your choice of method.
So, when should you use DXA or MRI? This blog post will go through the pros and cons of each, and when it might be more beneficical to use one over the other.
But first, what is body composition?
Historically, assessing body composition in clinical trials has referred to quantifying the proportion of weight loss that is fat versus that which is ‘fat-free mass’ (FFM). Today, however, it means moving beyond this dichotomy to characterize specific tissue compartments and their distinct physiological roles:
- Subcutaneous adipose tissue (SAT): adipose tissue depot that functions as an endocrine organ and as long-term energy storage
- Visceral adipose tissue (VAT): ectopic adipose tissue depot within the abdominal cavity, a major driver of metabolic dysfunction
- Other ectopic fat depots: lipids stored where they shouldn’t be – in and around organs such as the liver, kidneys, pancreas and heart
- Muscles: not just volumes, but also quality and composition with the presence of myosteatosis, intra- and intermuscular fat in or between the muscles
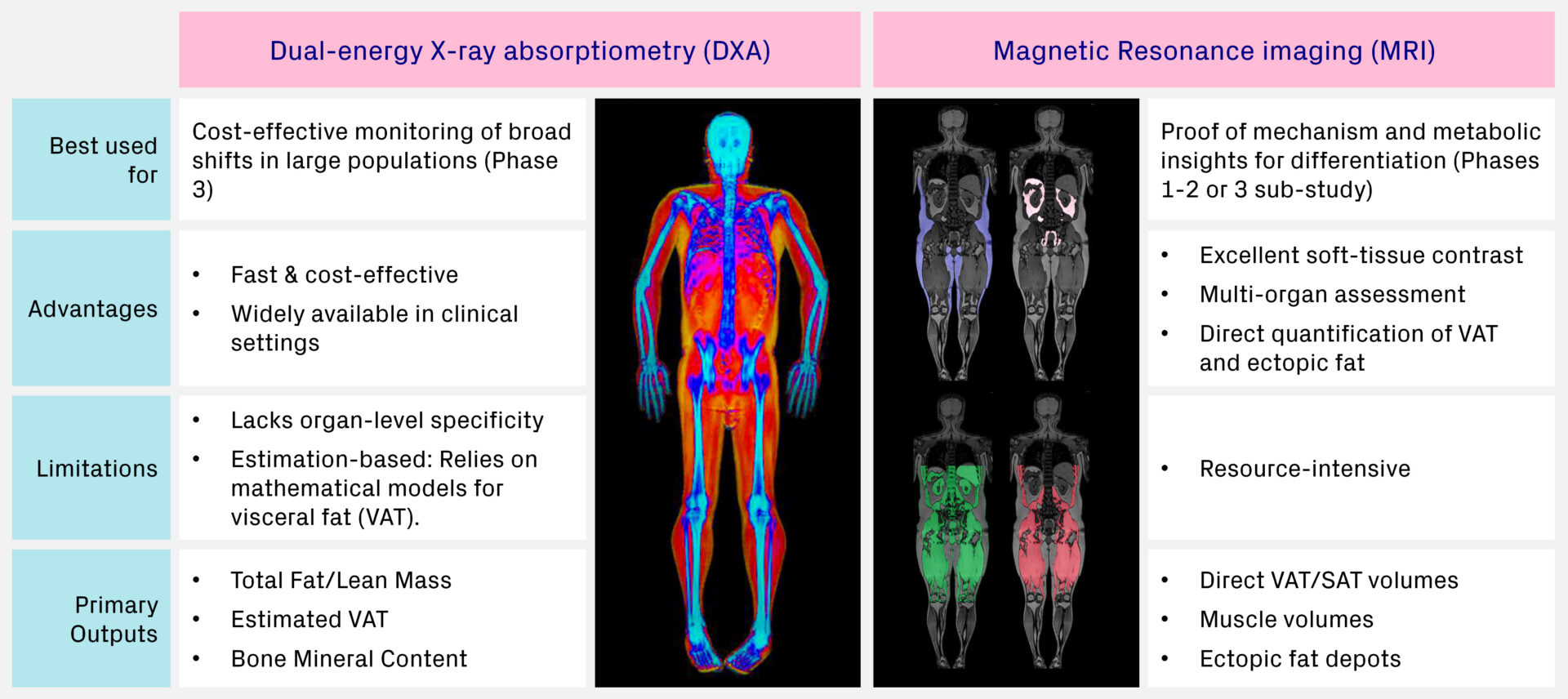
DXA: A practical choice for large-scale studies
Dual-energy X-ray absorptiometry (DXA) is the established standard for measuring bone mineral density (BMD), evaluating fracture risk, and diagnosing osteoporosis. By employing low-dose X-rays of varying energies, DXA effectively discriminates soft tissue from bone while also separating the soft tissue into fat mass (FM) and fat-free mass (FFM). Additionally, some DXA systems can provide an estimate of visceral adipose tissue (VAT), however, it is important to note that this relies on a calculation rather than a direct volumetric measurement.
Despite this limitation, DXA provides a solid foundation for assessing broader body composition changes over time. As a fast, accessible and cost-effective imaging method, it is particularly well-suited for large-scale clinical trials where the goal is to monitor general changes rather than highly detailed tissue characterization.
MRI: A precise and comprehensive view of body and muscle composition
Magnetic resonance imaging (MRI) uses a powerful magnetic field and radio waves to generate highly detailed tomographic images of the body’s internal structures. One of the key strengths of this technology is its ability to provide excellent soft tissue contrast, making it an ideal tool for examining individual organs, muscles, and other non-bony tissues.
MRI provides detailed volumetric assessments of fat and lean tissue compartments through quantification of SAT, VAT, adipose tissue-free volume and skeletal muscle volume from whole-body images. Crucially, MRI is the only imaging method capable of directly measuring changes in specific ectopic fat depots within organs such as the liver, kidney, heart, pancreas, and muscle.
For advanced muscle composition analysis, MRI enables categorization of the different types of muscle fat. At Antaros Medical, we segment all the thigh muscles individually, which enables us to quantify anf assess all adipose tissue within and around the muscle (intra- and inter-MAT). This is important in trials where changes over time matter and specificity is crucial. You can read more about our muscle composition assessment here.
When you need precise and accurate measures of different fat compartments and regional tissue characterizations to ensure that observed differences reflect true physiological changes rather than methodological variation, MRI is the best choice of method.
Strategic implications: Choosing DXA or MRI for an obesity clinical trial
Ultimately, the decision to implement DXA or MRI hinges on the specific research questions, protocol endpoints and the phase of your clinical program. DXA remains a pragmatic choice for large-scale Phase 3 trials where the primary goal is to monitor broad shifts in fat and lean mass across a large cohort of participants. However, as the obesity landscape shifts toward metabolic differentiation and functional improvements, MRI is becoming the method of choice for Phase 1 and 2 trials and Phase 3 sub-studies.
While DXA priovides a helpful ‘snapshot’ of body composition, it relies on estimates for visceral fat and cannot distinguish between different ectopic fat depots. In contrast, MRI can deliver direct evidence of and insights into changesin tissues like adipose tissue, liver, heart, kidney, and skeletal muscle.
It is also worth noting that although computed tomography (CT) is another available method, it is not frequently used in body composition due to its ionizing radiation. However, where it is the method of choice and alteady part of the trial protocol (e.g. in cardiology and oncology indications), body composition analysis can be added on opportunistically. Leveraging exisiting CT scans avoids the needs for additional imaging sessions, reducing patient burden, while still providing valuable insights into fat and muscle distribution.
Closing thoughts
Choosing the right imaging method to assess body composition and other end-organ endpoints in criticial, and it’s not one-size-fits-all. At Antaros Medical, we guide you in selecting the most suitable approach based on your trial phase, endpoints, and scientific objectives, ensuring your study captures what’s really underneath the lost kilos.
To summarize briefly what has been covered in this blog post:
- Beyond weight loss: Success in obesity drug development now hinges on proving ‘quality’ of weight loss, including improvements in metabolic resilience, organ health, and muscle quality.
- Diverse methodologies: While multiple imaging techniques are available for assessing body composition, each offers trade-offs in precision, level of detail and scalability.
- Strategic selection: There is no universal best method. Choosing the right imaging method depends entirely on the clinical trial phase, specific research objectives, and the primary endpoints required.
Blog disclaimer:
The views and opinions expressed in this article are solely those of the contributing author/s. These views and opinions do not necessarily represent those of Antaros Medical.
Contact details:
If you have any questions regarding this article, please reach out to press@antarosmedical.com